Hello and thanks for visiting my blog to learn more about optimizing your bone health! My name is Jen Birge and I’ve been fascinated with improving bone health since I was diagnosed with osteoporosis after having breast cancer in 2019. As a Nutritionist for Osteoporosis and Bone Health, I want to share what I’ve learned and what I continue to learn.
My breast cancer was estrogen positive so my treatment involved suppressing estrogen levels in my body which is not helpful for bone health. So, naturally, I started my journey of learning about bone health and doing what I can to optimize my own bone density and strength.
My goal is to share science-based information with you in a simple format that is easy to understand. But, first, I’d like to share more about my experience with osteoporosis.
While breast cancer treatment pushed me into the osteoporosis range of low bone density, there were other factors that definitely contributed. If you read on, I’ll explain how having Polycystic Ovarian Syndrome, Insulin Resistance and being paralyzed with a condition called Acute Disseminated Encephalomyelitis also contributed to me having lower bone density.
My Journey with Osteoporosis
Polycystic Ovarian Syndrome (PCOS):
Polycystic Ovarian Syndrome (PCOS) is complicated and involves a lot of different symptoms but when I was a teen, I didn’t have access to information that the internet provides us now. And, I didn’t know it was associated with osteoporosis.
In college, I finally went to the student health clinic for having a very irregular menstrual cycle and was told that if I ever have a hard time getting pregnant I should see a doctor. I was put on oral contraceptives to regulate my period and then when I was ready to start a family, I saw an endocrinologist and was given the PCOS diagnosis.
With PCOS, I had challenges with getting pregnant and it also increased my risk for insulin resistance and osteoporosis. Now I know there’s a connection with PCOS and osteoporosis as women with PCOS have been shown to have lower bone density (1).
Insulin Resistance
My very first job as a dietitian was at a diabetes self-management program where I became fascinated with insulin resistance (insulin helps our cells use glucose so being insulin resistant means our body doesn’t use insulin well and we might develop prediabetes or diabetes). I enjoyed working with people helping them either prevent diabetes and/or also best manage their diabetes
After having my second child and gaining too much weight, in my 30’s, I was shocked to learn I had prediabetes. Because of my experience, I knew what to do to get out of the prediabetes range. Since then I’ve always worked to keep a normal A1c and stay in the normal range (it’s possible!). Both grandparents on my mom’s side had diabetes, so I have a strong family history there. Like with PCOS, being insulin resistant also increases one’s risk for osteoporosis (2).
Auto-immune Condition: ADEM

In 2010 (my late 30’s), I developed an auto-immune condition, called Acute Disseminated Encephalomyelitis (ADEM) after visiting Thailand. It’s very rare and grouped with Multiple Sclerosis (MS) but, fortunately, it’s not progressive like MS. Since it’s “acute”, the damage it does is what you are left with and people have varying severity of residual symptoms.
I had brain damage from the brain swelling, was paralyzed from the waist down and in only 2 weeks, I lost 20 lbs, most of which I know was muscle! I had nerve damage and if muscle doesn’t have innervation, it goes quickly so I had to rebuild muscle AND learn to walk again. That definitely was not on my bucket list.
Maybe one day I’ll share more – this is a short version of the story but I was in a rehab for a month building muscle and learning to walk! It was the hardest thing I’ve ever done and, thankfully, I was able to leave rehab using a walker.
The photo I’m sharing is of me standing for the first time (with assistance!). It took months after that to recover and I still have to focus on improving my strength and balance.
None of my doctors or physical therapists discussed bone health with me but now I understand that my rapid weight and muscle loss during this time, along with a period of being immobile, also contributed to my risk for lower bone density. I wish I would have had a bone density scan during this time!
Breast Cancer with Estrogen Suppression
Then, later in my 40’s, I found out I had breast cancer and treatment included being put into menopause….pretty much overnight! Thankfully, I am a breast cancer survivor and I am very grateful for my health.
“Medical” menopause was a challenge and presented things like a sluggish metabolism, hot flashes, fatigue, brain fog, and poor sleep. And, because my cancer treatment involved estrogen suppression, this affected my bone health (3). When you have breast cancer, they do a bone density scan to establish a baseline so this is when I had my first bone density scan.
My baseline bone density revealed osteopenia, which is kind of the step or range before osteoporosis meaning your bone density scores are lower than normal but not low enough to be osteoporosis. I think my osteopenia developed because of the risk factors I already had – having PCOS, some insulin resistance and then being paralyzed and losing so much muscle very quickly.
Even then, no one recommended anything for my bone health and I was so focused on getting through treatment and preventing recurrence that I followed the oncology dietitian’s advice and adopted a mostly plant-based diet that was relatively low in protein (hint: that did NOT help my bone density). I wish I had been referred to a Nutritionist for Osteoporosis.
Then after treatment (radiation, having ovaries removed and estrogen suppressed) my next bone density scan, 2 years later, revealed some osteoporosis (left and right femoral neck, which is the top of the thigh bone). Since having breast cancer and the bone density scans, I’ve done a lot of my own research, and I’ve made A LOT of changes to improve my bone health. I’m due for another this year and excited to learn the results – I expect improvement back into the osteopenia range (at least!).
What I Focus On Now…
I know it can be scary to be diagnosed with low bone density (osteopenia or osteoporosis) but I feel that information is power and action is even more powerful. And, because it’s a silent condition not a lot of healthcare providers and dietitians give it the attention it deserves. This is why I’ve decided to focus on being a Nutritionist for Osteoporosis.
Some of the things that I’ve done to improve my bone density include increasing protein intake, getting more calcium from food and supplements, taking vitamin D, magnesium and other supplements. I mostly avoid processed foods and focus on foods that promote gut health, which is important for the absorption of nutrients.
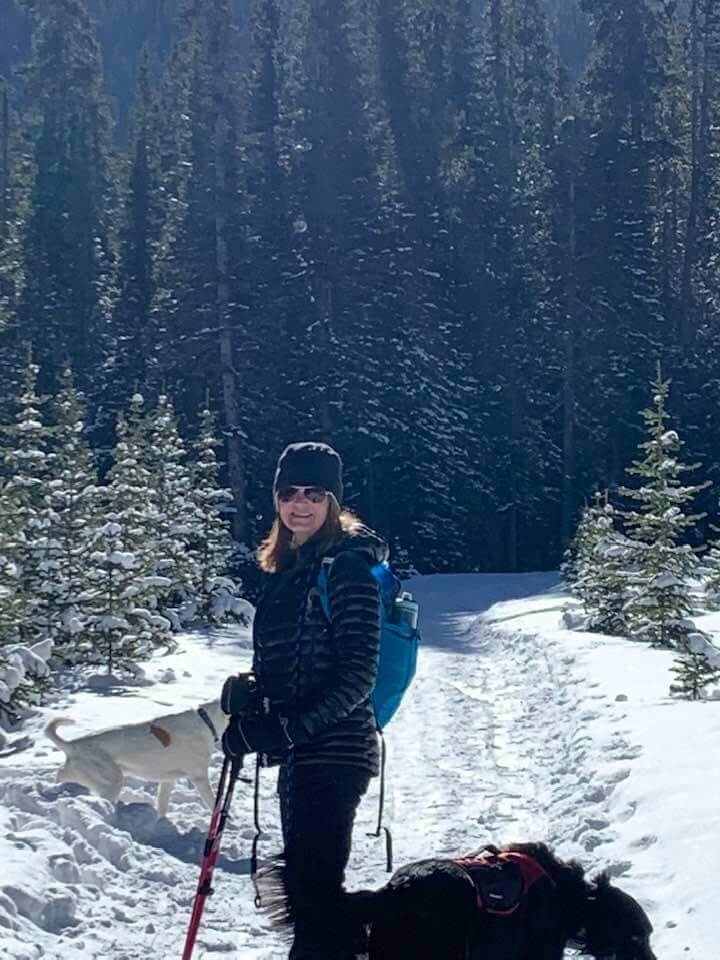
Weight-bearing exercise is key to bone health so I enjoy hiking and snowshoeing, often with a backpack or weighted vest. I practice some yoga for balance, lift weights and my newest activity is playing pickleball, which is very addictive!
I’ve also had two rounds of Reclast – a bisphosphonate infusion that works to slow down bone breakdown. I’m optimistic about my bone health and I look forward to my next bone density scan. I also look forward to sharing this information with anyone looking to strengthen their bones and reverse osteopenia or osteoporosis. I hope you keep reading as I share more information. If you have ideas or topics that you would like me to cover in future blog posts, please reach out to me with your ideas here.
Hugs,
Jen Birge, MS,RDN, CDCES
Nutritionist for Osteoporosis and Bone Health